Catholic Medical Quarterly Volume 71(1) February 2021
Faith in Medicine
The link between the Veil of Manoppello image and Christ’s shoulder wound.
Fr. Patrick Pullicino
Abstract
 The
Veil of Manoppello shows the face of the Rising Christ. Saint Padre Pio
called it the “greatest miracle in our possession”. The face on the veil
shows a right Horner’s syndrome. The possible origin of this was suggested
by Bevilacqua et al who photographed abrasions on the upper back of the
Turin shroud on both sides. They say that these resulted from a transfer
of Christ’s cross from his right to his left shoulder. Their research
shows that it is probable that Christ carried a T-shaped cross which had
supporting struts for the patibulum. They conclude that in a fall, Jesus’
right shoulder was trapped between a strut and the patibulum and he
suffered a right infra-glenoid shoulder dislocation. During forcible
lowering of the arm an extensive brachial
plexus injury resulted. Horner’s syndrome is typical for an inferior
brachial plexus traction injury.
The
Veil of Manoppello shows the face of the Rising Christ. Saint Padre Pio
called it the “greatest miracle in our possession”. The face on the veil
shows a right Horner’s syndrome. The possible origin of this was suggested
by Bevilacqua et al who photographed abrasions on the upper back of the
Turin shroud on both sides. They say that these resulted from a transfer
of Christ’s cross from his right to his left shoulder. Their research
shows that it is probable that Christ carried a T-shaped cross which had
supporting struts for the patibulum. They conclude that in a fall, Jesus’
right shoulder was trapped between a strut and the patibulum and he
suffered a right infra-glenoid shoulder dislocation. During forcible
lowering of the arm an extensive brachial
plexus injury resulted. Horner’s syndrome is typical for an inferior
brachial plexus traction injury.
The Veil of Manoppello is a diaphanous veil made of sea-silk with an image of the face of Christ during the Resurrection (figure 1). The eyes are open, but the face still shows bruises. It has been found to be super imposable on the shroud image of the face of Christ. The left pupil is miotic compared to the right and there is a slight ptosis – typical features of Horner’s syndrome due to sympathetic chain injury.
A recent paper by Bevilacqua et al(1) gives a possible explanation for the presence of the Horner’s syndrome. These authors noted bruises/scuff marks in four locations in the upper back area of the Turin shroud. They constructed an experimental cardboard t-shaped cross and found that the scuff marks corresponded to areas of contact of the cross on the upper back. They concluded that the cross Jesus carried was a t-shaped cross. They also noted that the upper mark (1, figure 2) was more evident on the right whereas the lower mark (4, figure 2) was more evident on the left. They concluded that Jesus first started carrying the cross on the right side, but later it was switched to the left, and his posture was more stooped probably as he was tiring.
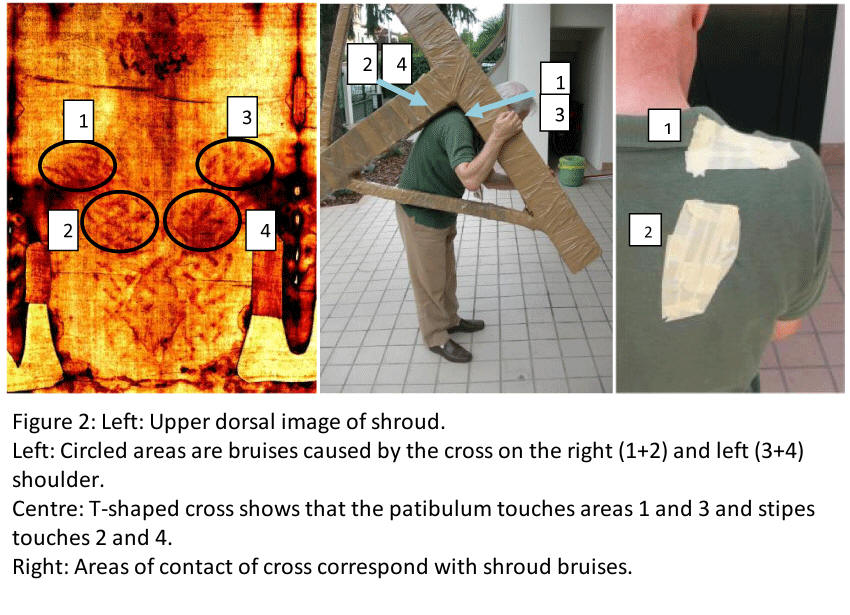
Bevilacqua et al also make measurements on the arms of the shroud image.(2) They find that the right arm reaches lower than the left, with the fingertips reaching the lateral thigh. They also found that the right humerus is 3.5 cm below the shoulder which they conclude is due to an infra-glenoid dislocation. The cause of this dislo-cation they feel, was likely due to a fall when the cross was being carried on Jesus’ right side. The fall caused the patibulum to strike the ground, Jesus fell forward and his shoulder became trapped between the strut and the patibulum (Figure 2). The cross then fell across his back causing a violent upward pulling of his arm and the dislocation. Their measurements also show that the whole right shoulder is depressed and they attribute this to loss of shoulder muscle power. The flexed position of the digits of the right hand in the shroud points to loss of power in the hand muscles. They say this points to an extensive brachial plexus traction injury. This was likely caused when soldiers forcibly lowered Jesus’ right arm which would have been stuck in an elevated position by the infra-glenoid dislocation.
Jesus would have suffered tremendous pain, not only from the tearing of muscular structures around the shoulder joint, but by the intense causalgia pain that results from brachial plexus traction injuries, which is particularly a deep pain in the axilla and shoulder region. His right arm likely became flail and this caused the switch of the cross to his left side.
Bevilacqua et al deduce the presence of a Horner’s syndrome based on what they take to be a right enophthalmos in the face on the shroud. However, enophthalmos is not a detectable feature of Horner’s syndrome in man.(3) Horner’s syndrome is a well-known feature of lower brachial plexus injuries that affect the T1 root however. (4) The presence of Horner’s syndrome affecting the right eye in the Veil of Manoppello, does therefore support the conclusion that Jesus sustained a lower brachial plexus avulsion injury.
Christ first told St Bernard of Clairvaux about his shoulder wound when St Bernard asked him what was his greatest unrecorded suffering. St Bernard said that Christ told him: “I had on My Shoulder, while I bore My Cross on the Way of Sorrows, a grievous Wound which was more painful than the others and which is not recorded by men."
Padre Pio had a great devotion to this wound and it has been thought that the wound was caused by the heavy cross cutting into Christ’s shoulder, but no deep wound is seen on the shroud. The probable cause of the pain is therefore causalgia from brachial plexus avulsion. Causalgia (also called reflex sympathetic dystrophy) is the most severe pain known to humans and may lead to suicide. A sufferer, Chantele Baxter said of it “It is like being dipped in boiling oil. I had no idea the human body was even capable of producing that much pain.”
Jesus asked the faithful to honour his shoulder wound. He said to St Bernard: “honour this Wound with thy devotion and I will grant thee whatsoever thou dost ask through Its virtue and merit. And in regard to all those who shall venerate this Wound, I will remit to them all their venial sins and will no longer remember their mortal sins."
References
- Bevilacqua M, Fanti G, D’Arienzo M (2017) New Light on the Sufferings and the Burial of the Turin Shroud Man. Open J Trauma 1(2): 047-053.
- Bevilacqua M, Fanti G, D’Arienzo M, De Caro D. (2014) Do we really need new medical information about the Turin Shroud? Injury. Int. J. Care Injured 45 460–464.
- Patten J. (1996) Neurological Differential Diagnosis. Springer, London, p12.
- Patten J. (1996) Ibid, p. 12.